Knee Arthroscopy
Knee arthroscopy is a surgical procedure that allows doctors to view the knee joint without making a large incision (cut) through the skin and other soft tissues. Arthroscopy is used to diagnose and treat a wide range of knee problems.
During knee arthroscopy, your surgeon inserts a small camera, called an arthroscope, into your knee joint. The camera displays pictures on a video monitor, and your surgeon uses these images to guide miniature surgical instruments.
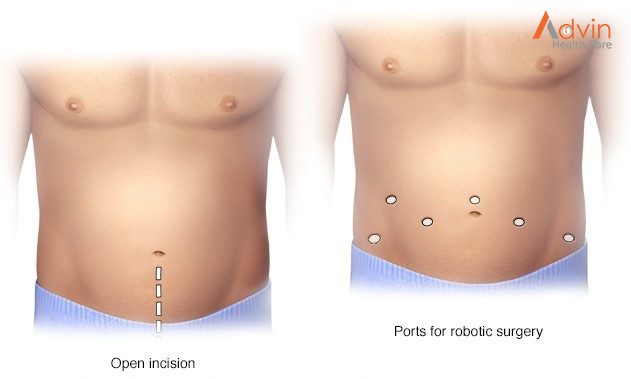
Because the arthroscope and surgical instruments are thin, your surgeon can use very small incisions, rather than the larger incision needed for open surgery. This results in less pain and joint stiffness for patients, and often shortens the time it takes to recover and return to favourite activities.
Your knee is the largest joint in your body and one of the most complex. The bones that make up the knee include the lower end of the femur (thighbone), the upper end of the tibia (shinbone), and the patella (kneecap).
Other important structures that make up the knee joint include:
- Articular cartilage.The ends of the femur and tibia, and the back of the patella are covered with articular cartilage. This slippery substance helps your knee bones glide smoothly across each other as you bend or straighten your leg.
- The knee joint is surrounded by a thin lining called synovium. This lining releases a fluid that lubricates the cartilage and reduces friction during movement.
- Two wedge-shaped pieces of meniscal cartilage between the femur and tibia act as shock absorbers. Different from articular cartilage, the meniscus is tough and rubbery to help cushion and stabilize the joint.
- Bones are connected to other bones by ligaments. The four main ligaments in your knee act like strong ropes to hold the bones together and keep your knee stable.
- The two collateral ligaments are found on either side of your knee.
- The two cruciate ligaments are found inside your knee joint. They cross each other to form an X with the anterior cruciate ligament in front and the posterior cruciate ligament in back.
Who needs knee arthroscopy?
Your healthcare provider may recommend knee arthroscopy if you have knee pain that doesn’t get better with nonsurgical treatments. Nonsurgical treatments include rest, ice, nonsteroidal anti-inflammatory drugs and physical therapy (PT). Although arthritis causes knee pain, arthroscopic knee surgery isn’t always an effective treatment for osteoarthritis.
Healthcare providers use arthroscopy to get a better look at cartilage, bones and soft tissues inside of your knee. They use the procedure to diagnose several types of knee injuries. Most of these injuries affect ligaments and cartilage in your knee joint.
Knee injuries among athletes (including adolescents) are very common. They can happen in contact sports and those that require jumping, such as volleyball.
What happens during knee arthroscopy?

During the procedure, your healthcare provider:
- Cleans your leg and secures your knee in a stabilizing device. The device ensures that your knee stays in the proper position throughout the procedure.
- Makes a small incision (cut) in your knee and inserts a long metal tool called an arthroscope into the incision. The arthroscope has a camera on the end. Images from the camera appear on a screen in the operating room.
- Looks at the images on the monitor and uses them to diagnose injuries and guide the procedure. If you need surgery, your healthcare provider makes other incisions in your knee and inserts tiny tools through them.
- Repairs torn tissues, shaves off damaged bone or cartilage and removes inflamed or damaged tissues. Your healthcare provider uses specially designed tools for these tasks.
- Closes the incisions with stitches or small bandages, and wraps your knee with a larger bandage or dressing.
What are the advantages of knee arthroscopy?
Minimally invasive procedures like knee arthroscopy usually require less recovery time than traditional (open) surgery. As you only need a few small stitches, you’re more likely to get back on your feet more quickly than with traditional surgery. You may also have less pain and a lower risk of infection.